florida blue appeal form
Mail the form and supporting documentation to. Health coverage is offered.

Insurer Prevails On Appeal In Florida Assignment Of Benefits Case Propertycasualty360
When submitting a provider appeal please complete the form in its entirety in accordance with the instructions contained in Florida Blues Manual for Physician and Providers available online.
. The following tips will allow you to fill out Provider Appeal Form Instructions - Florida Blue quickly and easily. Please send only one claim per form. Date _____ Provider Reconsideration Administrative Appeal must.
Jacksonville FL 32203-3237. Open the form in our feature-rich online editing tool by clicking on Get form. ROC 10C Miami Florida 331221932 Jacksonville Florida 32202 Fax 3054377490 Fax 3054377490 REQUEST FOR REVIEW I HEREBY request a review of the grievance described.
Florida BlueFlorida Blue HMO PO Box 41609 Jacksonville FL 32203 -1609 Attn. Appeal Florida BlueFlorida Blue HMO may need medical or other records for information relevant to my Grievance or Appeal. Find all your forms for prescriptions claims and more all right here.
Appeal Florida Blue Preferred HMO may need medical or other records for information relevant to my Grievance or Appeal. Florida BlueFlorida Blue HMO PO Box 41629 Jacksonville FL 32203-1629 Attn. Blue Cross and Blue Shield of Florida.
Florida Blue Health Plan Grievance And Appeal Form The correctness in the information and facts offered about the Overall health Strategy Develop is essential. Health Plan Grievance Appeal Form Non. 835 Health Care Electronic Remittance Advice Request Form.
Discover all the ways members can earn wellness incentives and rewards for taking an active role in their health. Accredo Prescription Enrollment Form. Accordingly I authorize those persons or entities that have.
You can ask us to reconsider by filing a grievance with us. Adult Problem List. Member Grievance and Appeal Form Mail to.
BlueMedicare HMOPPORPPO Member Grievance and Appeal Form Mail to Florida BlueFlorida Blue HMO PO Box 41609 Jacksonville FL 32203-1609 Attn Medicare Advantage Member. You can look in your Evidence of Coverage for information about how to file a grievance contact us at 1-800-926. Accordingly I authorize those persons or entities that have any.
Medicare Advantage Member Appeals and Grievances. Florida Blue members take full advantage of your insurance plan. Ancillary Request to Participate Form.
Medicare Advantage Member Grievances Appeals Fax. Appeals must be submitted within one year from the date on the remittance advice. Provider Disputes Department.
Date _____ Provider Reconsideration Administrative Appeal must. Member Grievance and Appeal Form. Please send only one claim per form.
This address is intended. Get rewarded for healthy behaviors. Appeals must be submitted within one year from the date on the remittance advice.
I hereby request a review of the Appeal or Grievance described below and understand that the receipt of this Appeal and Grievance Form by Florida Blue constitutes a request for review by.

Rogers Benefit Group Florida Fill Online Printable Fillable Blank Pdffiller
Welcome Home Bienvenidos A Casa Our Lady Of Lourdes

Provider Appeal Form Instructions Florida Blue Fill And Sign Printable Template Online Us Legal Forms

Tropical Storm Ian Spaghetti Models
Starting An Academic Appeal Uwf Public Knowledge Base Uwf Confluence

Tropical Depression 12 Forms In East Atlantic Wfla
![]()
Welcome To The Tampa Housing Authority

News Press Releases Florida Farm Bureau
![]()
Know Your Court Florida Courts
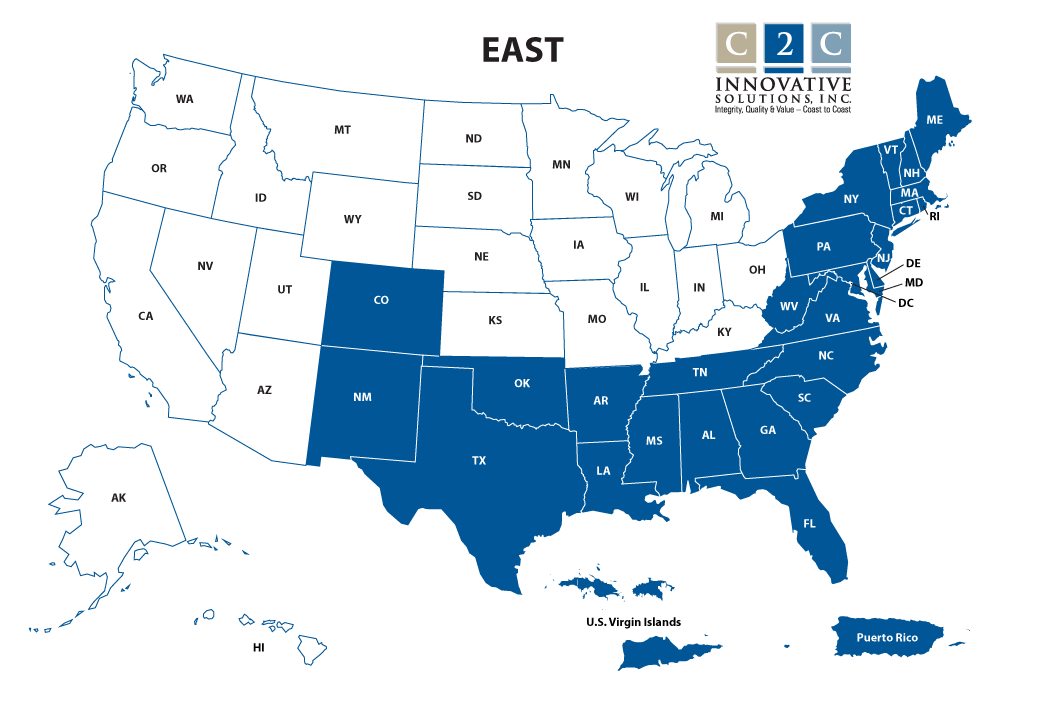
Qic Part A East
Florida Health Insurance Marketplace 2022 Guide Healthinsurance Org
![]()
File A Claim Aflac

2022 Voter Guide Duval County Democratic Party

Florida Blue Appeal Fax Number Fill Online Printable Fillable Blank Pdffiller

Emergency Rental And Utility Assistance Program
Florida S Unemployment System Your Questions Answered
Tax Information Floridajobs Org

Update New Certificates Of Medical Necessity Medical Florida Blue

Florida Blue Key Wikipedia